GLP-1 Receptor Agonists for Weight Loss: How It Works, Benefits & Risks (2026 Guide)
The landscape of metabolic health has changed forever. In 2026, we no longer view obesity simply as a failure of willpower, but as a complex hormonal challenge. At the heart of this medical revolution is the GLP-1 receptor agonists for weight loss. Once a quiet breakthrough in type 2 diabetes care, these medications—part of a class known as incretin-based therapy—have become the gold standard for chronic weight management.
By mimicking the body’s natural signaling system, GLP-1 receptor agonists (GLP-1 RAs) offer a high level of effectiveness, with some newer variants helping patients shed over 25% of their body weight. However, as their popularity surges, understanding the safety profile, FDA-approved uses, and the biological “why” behind their success is critical for anyone considering this journey.
What Is a GLP-1 Receptor Agonist?
To understand these drugs, we first have to understand the body’s communication system.
What Does “Receptor Agonist” Mean?
In medical terms, an agonist is a substance that attaches to a specific cell receptor and triggers a biological response.
Mimics Natural GLP-1: Your body naturally produces Glucagon-like peptide-1 (GLP-1) in the gut after you eat.
Activates Receptors: The medication “plugs into” the GLP-1 receptors in your brain, pancreas, and stomach.
Longer Half-Life: While natural GLP-1 lasts only minutes, pharmaceutical analogues are engineered to resist breakdown, staying active in your system for a full week.
How GLP-1 Works in the Body
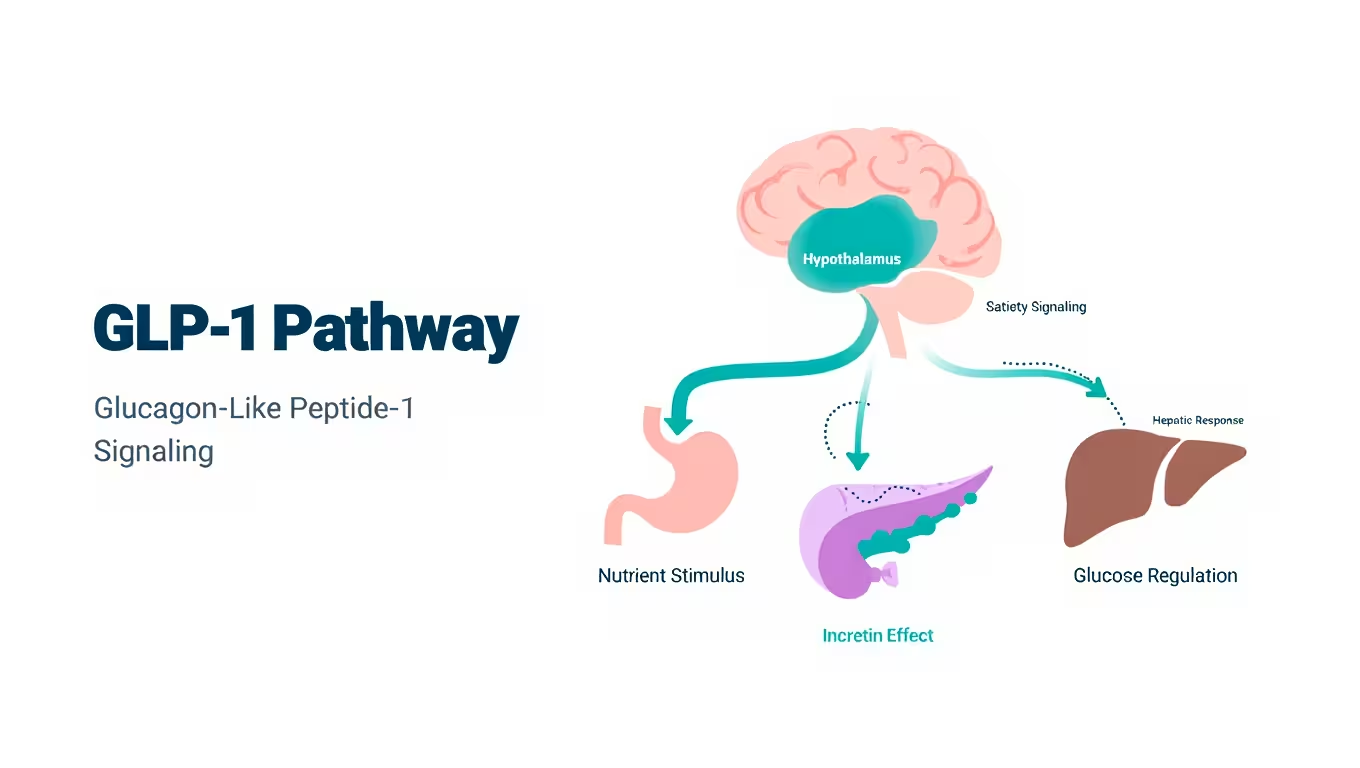
GLP-1 receptor agonists orchestrate a three-pronged metabolic strategy:
1. Stimulates Insulin Secretion: It tells the pancreas to release insulin, but only when blood sugar is high.
2. Reduces Glucagon: It prevents the liver from pumping out extra sugar into your bloodstream.
3. Slows Gastric Emptying: It physically keeps food in your stomach longer.
4. Hypothalamus Signaling: It crosses the blood-brain barrier to target the hypothalamus, effectively silencing the “food noise” or constant hunger signals.
How GLP-1 Receptor Agonists Cause Weight Loss
Weight loss on a GLP-1 RA isn’t just about eating less; it’s about changing how your body reacts to energy.
Appetite Suppression

By targeting the brain’s reward centers, these drugs reduce the “hedonic” drive to eat. You may find that foods you once craved no longer hold the same power over you.
Reduced Caloric Intake
Because food stays in your stomach longer (delayed gastric emptying), you feel physically full on much smaller portions. This creates a natural, sustainable calorie deficit without the typical “starvation” signals.
Improved Insulin Sensitivity
Many people with obesity suffer from insulin resistance, where the body’s cells ignore insulin. GLP-1s help reset this sensitivity, allowing your body to use stored fat for fuel more efficiently.
Effects on Metabolic Adaptation
When you diet traditionally, your metabolism often slows down (thermogenesis). GLP-1 RAs help stabilize metabolic rate, making it easier to maintain weight loss compared to calorie restriction alone.
FDA-Approved GLP-1 Receptor Agonists for Weight Loss
As of 2026, two primary “pure” GLP-1 receptor agonists are approved specifically for weight management.
Semaglutide (Brand: Wegovy)
Wegovy is the most widely prescribed weekly injection for obesity.
Effectiveness: Clinical trials show an average weight loss of 15–17% over 68 weeks.
Convenience: A once-weekly injection under the skin.
Liraglutide (Brand: Saxenda)
Saxenda was the first major GLP-1 approved for obesity.
Dosing: It requires a daily injection.
Effectiveness: Average weight loss is around 8–10%.
Note: While less potent than Semaglutide, it is often used by patients who want a drug that leaves their system quickly if they experience side effects.
🔗 Compare all drugs: Best GLP-1 Drugs for Weight Loss (2026 Comparison)
GLP-1 Receptor Agonist vs. GLP-1/GIP Dual Agonist
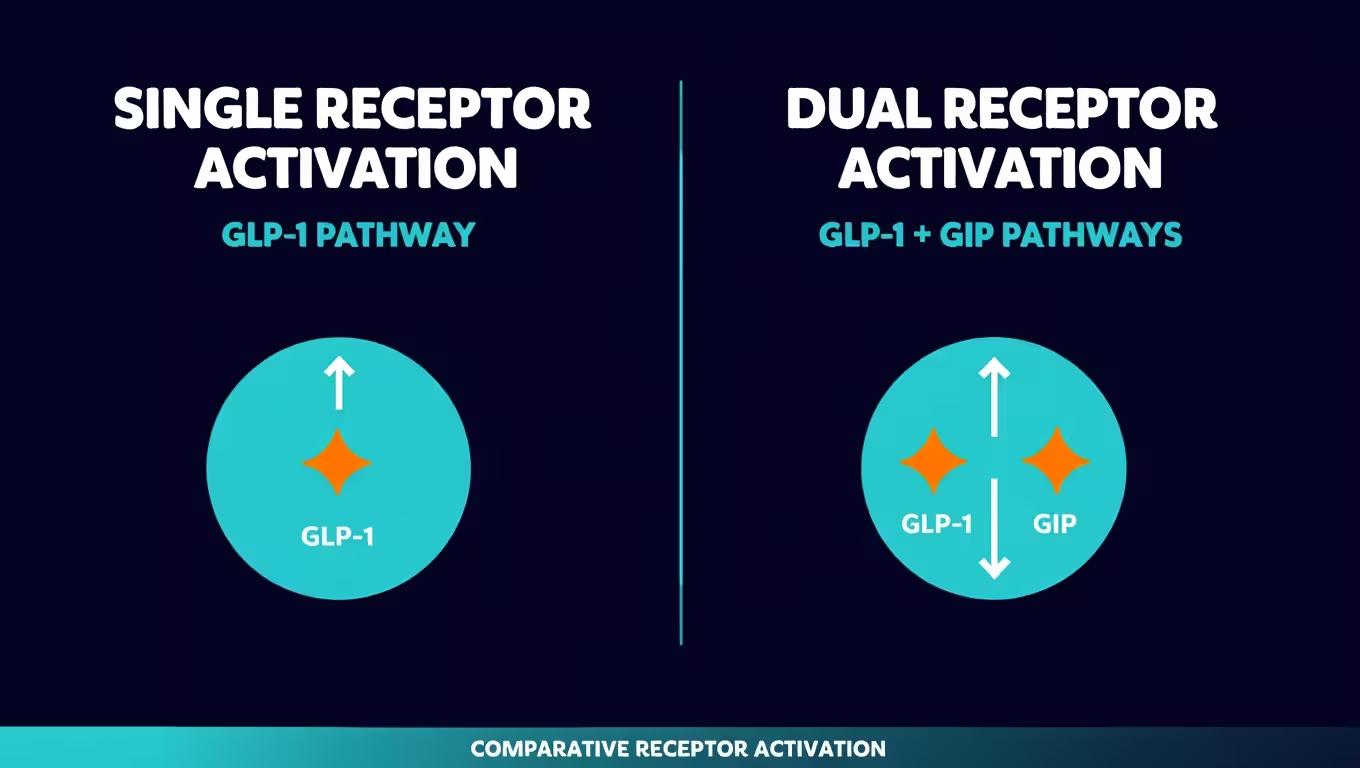
In 2026, the biggest debate is whether to use a “single” or “dual” agonist.
Single Agonists (Wegovy): Target only the GLP-1 receptor.
Dual Agonists (Zepbound/Tirzepatide): Target both GLP-1 and GIP (Glucose-dependent insulinotropic polypeptide).
Why Dual Agonists often outperform: By adding GIP, medications like Tirzepatide achieve higher weight loss—averaging 21% to 25.5% in recent 2026 data 1. Additionally, GIP may help reduce the nausea that some experience with pure GLP-1 drugs.
How Effective Are GLP-1 Receptor Agonists?

Average Weight Loss in Clinical Trials
3 Months: 5-8% of total body weight.
6 Months: 10-15% of total body weight.
12 Months: 15-22% (depending on the specific drug used).
Real-World Data vs. Clinical Trials
Real-world data in 2026 shows that while weight loss is slightly lower than in tightly controlled trials (often due to inconsistent dosing), the cardiovascular benefits—such as reduced blood pressure and lower stroke risk—are even more significant than initially predicted.
Side Effects and Safety Profile

Common Side Effects
Most side effects occur when you first start the medication or increase your dose:
Nausea & Vomiting: Usually subsides after 4-8 weeks.
Constipation: A result of the “slowed stomach” effect.
Diarrhea: More common with dual agonists.
Serious but Rare Risks
Pancreatitis: Inflammation of the pancreas.
Thyroid Warning: People with a family history of Medullary Thyroid Carcinoma should avoid these drugs.
Gallbladder Disease: Rapid weight loss can lead to gallstones.
Lean Mass & Muscle Loss Concerns

A major clinical focus in 2026 is Sarcopenia. When you lose weight rapidly, your body may burn muscle instead of fat. To prevent this, experts recommend a high-protein diet (1.2g+ per kg of body weight) and at least two days of resistance training per week.
🔗 Dosage & Titration Guide: How to Minimize GLP-1 Side Effects
Who Is Eligible for GLP-1 Receptor Agonist Therapy?
According to 2026 medical guidelines, eligibility is typically based on:
BMI of 30 or higher (Obesity).
BMI of 27 or higher (Overweight) with at least one weight-related condition like hypertension or sleep apnea.
Non-Diabetics: You do not need to have diabetes to use these medications for weight loss.
Cost and Insurance Coverage
The cost of a brand-name GLP-1 receptor agonist for weight loss is approximately $900–$1,300 per month out-of-pocket.
Insurance: In 2026, many plans require “Prior Authorization.”
Compounded Options: Many patients use reputable compounding pharmacies to access Semaglutide for $179–$299 per month.
🔗 Detailed Cost Guide: GLP-1 Weight Loss Cost & Insurance Coverage
What Happens If You Stop a GLP-1 Receptor Agonist?

Obesity is now viewed as a chronic condition. Clinical data shows that if you stop the medication without a long-term maintenance strategy, the body’s hormonal signals (ghrelin) will return, often leading to weight regain of up to two-thirds of the lost weight within a year.
Most providers now recommend a “maintenance dose” or a very slow “tapering” process combined with intensive lifestyle changes.
Frequently Asked Questions
What is the strongest GLP-1 receptor agonist?
Currently, Tirzepatide (Zepbound) is the most potent approved option. However, Retatrutide is a triple agonist in 2026 trials showing nearly 30% weight loss.
Is semaglutide a GLP-1 receptor agonist?
Yes, Semaglutide (Wegovy/Ozempic) is the prototypical GLP-1 receptor agonist.
Are these safe long term?
Studies through 2026 show significant benefits for heart and kidney health, though long-term use requires monitoring of bone density and muscle mass.
Final Verdict – Are GLP-1 Receptor Agonists Worth It?

If you have struggled with chronic obesity and metabolic syndrome, GLP-1 receptor agonists are a revolutionary, life-changing tool. They aren’t a “cheat code”—they are a biological correction.
However, they work best when combined with:
High Protein Intake to save muscle.
Strength Training to maintain metabolism.
Medical Supervision to manage dosage and side effects.
Consult with a board-certified obesity specialist to see if a GLP-1 RA is the right path for your metabolic health.

Reliable Health Insights, Expert Medical Guidance, Updates, Tools, and Valuable Resources.




Stay informed with valuable health and wellness tips delivered straight to your inbox.
Created with ©systeme.io